Shopping Cart
No item in your cart!
RM0.00
Scoliosis is a three-dimensional deformity of the spine characterised by an abnormal lateral curvature — forming a C-shaped or S-shaped curve when viewed from behind. It can affect people of all ages, from children and adolescents during periods of rapid growth, through to adults as a result of age-related spinal degeneration.
While mild cases may require only monitoring, more significant curves can affect posture, breathing, and quality of life — and in selected cases, surgical correction may be the most appropriate pathway. Earlier detection and diagnosis allows early conservative treatment such as bracing — which can avoid unnecessary surgery and preserve a higher health-related quality of life.
Scoliosis does not always cause pain — particularly in its early stages. In many cases it is first noticed through a visible change in posture or body symmetry rather than discomfort. Recognising the early signs is important because earlier intervention produces better outcomes.
Physical signs to look out for:
Scoliosis is not a single condition — it presents in different forms depending on the cause, age of onset, and severity of the spinal curve. Understanding the type of scoliosis is the first step towards determining the most appropriate treatment pathway.
The most common form of scoliosis, typically developing during the adolescent growth spurt between the ages of 10 and 18. Adolescent idiopathic scoliosis affects nearly 80% of idiopathic scoliosis cases and usually develops during rapid growth phases, requiring close observation. Skoliosis The cause is unknown — reflected in the term "idiopathic" — but the condition tends to be more prevalent and progress more rapidly in girls. Most cases are mild and can be monitored or managed with bracing, with surgery considered when curves are severe or continue to progress.
In adults, scoliosis can develop as a result of age-related spinal degeneration — disc wear, joint breakdown, and changes in spinal alignment that accumulate over time. Unlike adolescent scoliosis which is linked to growth, adult degenerative scoliosis is driven by the gradual deterioration of spinal structures and can cause significant back pain, nerve compression, and reduced mobility in older patients.
Caused by abnormal development of the spine during the embryonic stage — resulting in vertebrae that are malformed, incompletely formed, or fused together. Congenital scoliosis is usually identified at birth or in early infancy and often requires surgical correction, particularly in cases of severe or rapidly progressing curves.
Occurs as a secondary result of conditions affecting the nerves or muscles that support the spine — such as cerebral palsy, muscular dystrophy, or spinal muscular atrophy. Management is tailored to both the scoliosis and the underlying condition, and surgical correction is often required in more advanced cases.
Accurate diagnosis is the foundation of effective scoliosis management. At Sunway Medical Centre Penang, scoliosis assessment follows a structured process — combining clinical examination with appropriate diagnostic imaging to confirm the diagnosis, assess the severity of the curve, and plan the most appropriate treatment pathway.
The initial assessment involves a thorough physical examination — including the Adam's Forward Bending Test, where the patient bends forward at the waist while the examiner observes the spine for asymmetry or a rib hump. A scoliometer may be used to measure the angle of trunk rotation. Neurological assessment is also performed to identify any nerve involvement, particularly in adult patients.
The Cobb angle measurement is the internationally recognised standard for classifying scoliosis severity — with curves above 10 degrees confirming a diagnosis, and curves above 40 to 50 degrees generally indicating that surgery may be required.
Treatment depends on the type of scoliosis, the severity of the curve, the patient's age and growth stage, and whether the curve is progressing. Not all scoliosis requires surgery — and the goal of treatment is always to achieve the best possible outcome with the least invasive approach appropriate for the individual patient.
For mild curves — typically below 20 to 25 degrees — the primary approach is regular monitoring through clinical assessment and periodic X-rays. Many mild curves in adolescents do not progress significantly and do not require active intervention. The frequency of monitoring is determined by the patient's age, growth stage, and curve characteristics.
Specific exercise programmes — including Schroth Method physiotherapy and scoliosis-specific exercise approaches — can support postural correction, strengthen the muscles supporting the spine, and in some cases reduce curve progression. Physiotherapy is most effective when integrated with bracing or monitoring as part of a structured management plan.
For curves between 20 and 40 degrees in growing adolescents, bracing is the primary non-surgical intervention. A customised spinal brace is worn for a prescribed number of hours per day to prevent curve progression during the growth period. Bracing does not reverse an existing curve but is effective at preventing it from worsening — reducing the likelihood that surgery will be required.
Surgery is considered when curves are above 40 to 50 degrees, when a curve is progressing despite bracing, or when the deformity is causing significant functional impairment, pain, or respiratory compromise. The goal of scoliosis surgery is to straighten the spine as much as safely possible, prevent further progression, and maintain spinal balance and alignment for the long term.
At Sunway Medical Centre Penang, scoliosis surgery is supported by the Medtronic O-arm™ O2 Imaging System and StealthStation™ S8 Navigation System — the first in the northern region outside Klang Valley in Peninsular Malaysia.
The O-arm™ O2 captures real-time 3D images of the spine while the patient remains on the operating table — providing the surgical team with the most accurate and up-to-date view of the patient's anatomy at every stage of the procedure. This eliminates the need to transfer the patient to a separate imaging suite during surgery, reducing operative time and improving overall efficiency.
Working in conjunction with the O-arm™ O2, the StealthStation™ S8 acts as a surgical GPS — tracking the position of every surgical instrument in real time and displaying their exact location relative to the patient's spinal anatomy on a digital screen. This allows the surgeon to place pedicle screws and corrective implants with confidence, even in complex or severely rotated spines where anatomy may be significantly distorted.
Published clinical outcomes from this combined system include:
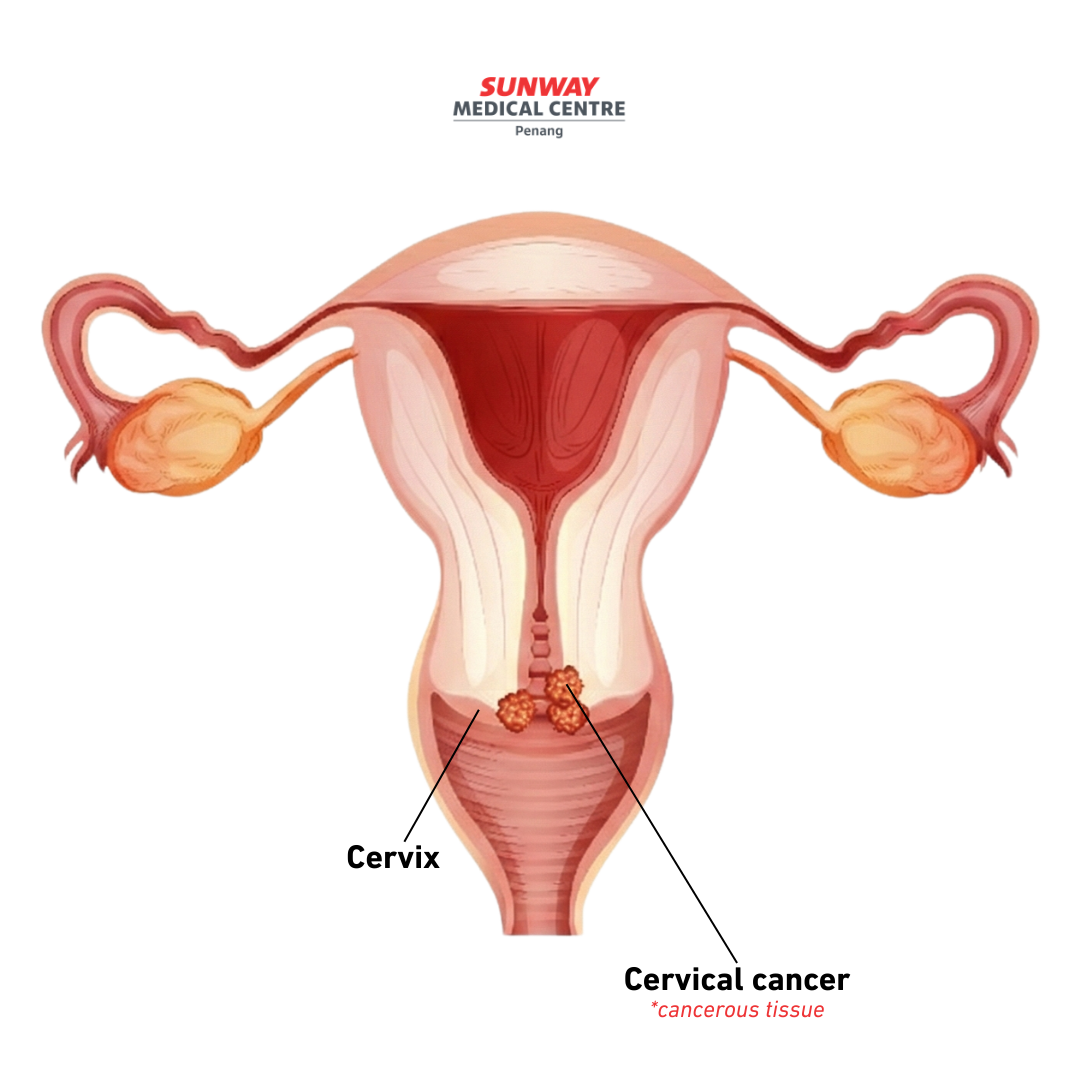
Cervical cancer often shows no early symptoms, which is why screening matters — even when you feel completely fine. Early detection can identify cervical cell changes before they become serious.
Take the next step — book a cervical cancer screening at Sunway Medical Centre Penang.
.png)